Recently, doctor Brian Broderick of Hopkins Hospital advocated an alternative to mechanical respiratory propulsion in the treatment of covar19: prone position combined with the use of nasal cannulas delivering oxygen at high flow rates (HFNC) is a strategy to prevent intubation and its complications in patients with moderate to severe acute respiratory distress syndrome (ARDS). Broderick warns that more data is needed to assess safety and efficacy.
March 30th 2020
Brian Broderick, MD:
(1) After caring for patients in the ICU with #COVID for the last week, the time seems right for a #pulmonology narrative on #Proning or #PronePositioning
(2) Let’s begin with a question: how does prone positioning improve oxygenation in patients with severe Acute Respiratory Distress Syndrome (ARDS)?
(3) First, some history. Prone positioning was first proposed in the 1970’s as a method to improve gas exchange in resp. failure and has long been shown to improve PaO2/FiO2 in mechanically ventilated patients with severe ARDS.
ncbi.nlm.nih.gov/pubmed/?term=1253612
ncbi.nlm.nih.gov/pubmed/3383620
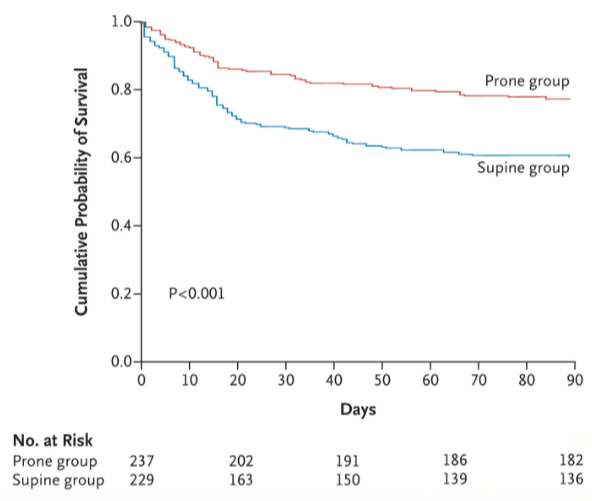
(4) However, translating physiologic improvements into clinical benefit proved challenging. It wasn’t until the NEJM PROSEVA trial that prone positioning became widely accepted as an effective therapy to reduce mortality in severe ARDS.
ncbi.nlm.nih.gov/pubmed/23688302
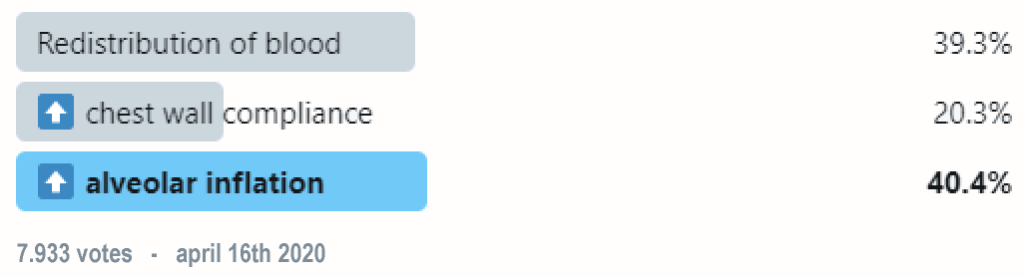
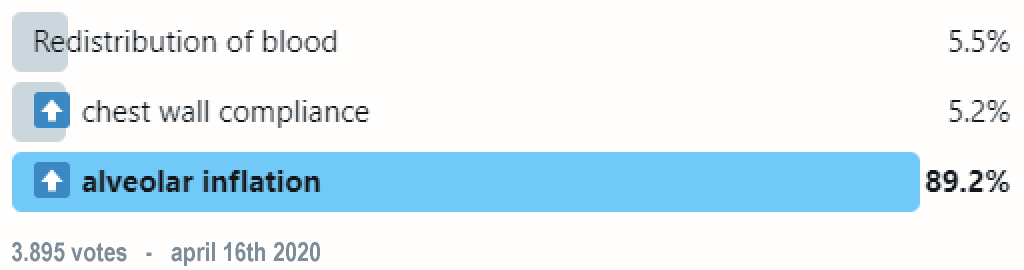
(5) That all sounds great, but how does prone positioning improve oxygenation? Well, a few theories exist:
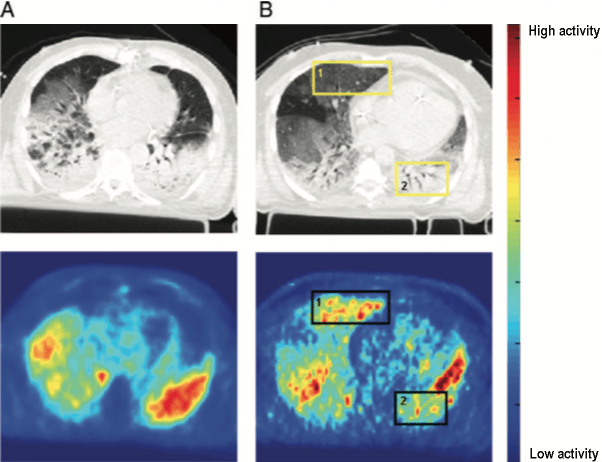
(6) First, let’s look at redistribution of blood flow. Studies in animals and humans (using PET) have shown that blood flow distribution in the lung does not change substantially from supine to prone position in ARDS.
ncbi.nlm.nih.gov/pubmed/2347780
ncbi.nlm.nih.gov/pubmed/19487931
(7) How about increased chest wall compliance? The dorsal chest wall is actually LESS compliant than the ventral chest wall, which leads to an overall net decrease in chest wall compliance when prone since the ventral wall is impeded from expanding.
ncbi.nlm.nih.gov/pubmed/?term=8111603
(8) Which leads us to our third theory: more uniform alveolar inflation! Anatomically speaking, lung mass is greater in the dorsal regions than the ventral regions.
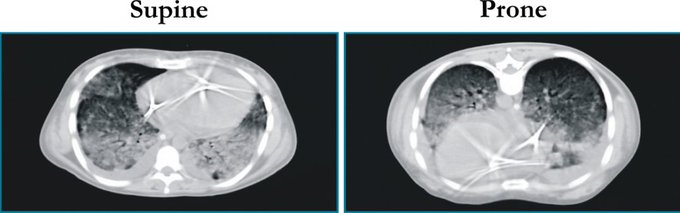
(9) When supine, there is greater distension of the ventral lung regions due to gravity, as well as poor “shape matching” between the lung and chest wall (think of a cone inside a cylinder).
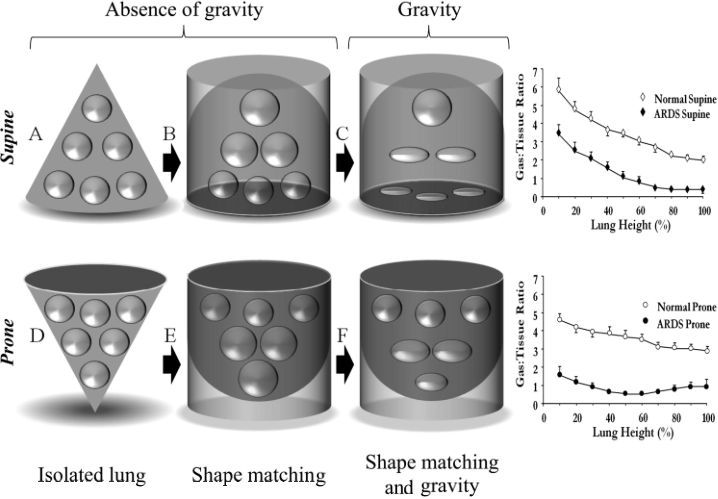
(10) When prone, the forces of gravity and “shape matching” oppose each other, which leads to more homogenous inflation of the pulmonary units from the sternum to vertebra.
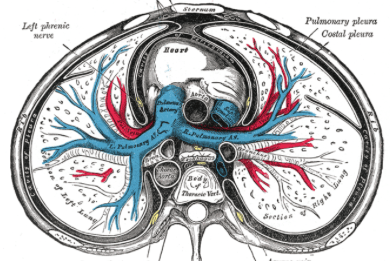
(11) Additionally, the heart weight no longer compresses the left lower lobe and abdominal pressure is lessened.
(12) This leads to an overall recruitment in (larger) dorsal lung regions which outweighs the degree of de-recruitment in the (smaller) ventral lung regions, leading to an overall increase in lung compliance.
ncbi.nlm.nih.gov/pubmed/?term=24134414
(13) This also explains why we do not typically see an increase in Pplat (during VC vent.) or a decrease in TV (during PC vent.) following pronation. Prone positioning also helps protect against Vent. Induced Lung Injury (VILI) by distributing stress and strain more homogeneously through the lung
(14) Here is a video courtesy of NEJM outlining the steps for prone positioning in mechanically ventilated patients (experienced staff is key!):
(15) So why is prone positioning so important in the #COVID pandemic? Based on clinical characteristic data from Wuhan, COVID often leads to ICU admission (15-20% of patients), ARDS (20% of patients), and mechanical ventilation (3% of patients).
ncbi.nlm.nih.gov/pubmed/?term=32109013
(16) In this last week alone, our team has pronated more patients than I have in my entire residency (with good results!)
(17) Interestingly, small prospective cohort studies have showed that prone positioning combined with HFNC (or NIV) in patients with moderate ARDS (PaO2/FiO2 > 100) may help avoid intubation.
ncbi.nlm.nih.gov/pubmed/?term=3000806
(18) Our experience in COVID patients has been similar. While still in the early stages of data collection, prone positioning in patients not mechanically ventilated seems to improve oxygenation, tachypnea, and dyspnea.

(19) With a looming shortage of vents, prone positioning with HFNC is a possible strategy to avoid intubation & its complications in patients with mod-to-severe ARDS, but more data is needed to assess safety & efficacy.
(20) So let’s revisit our original question: why does prone positioning improve oxygenation in patients with severe Acute Respiratory Distress Syndrome (ARDS)?
(21) SUMMARY:
✅ Prone positioning (PP) leads to more homogenous inflation of lungs
✅ This improves oxygenation, and reduces mortality in severe ARDS
✅ HFNC & PP is a possible strategy to consider to avoid intubation (especially in COVID pandemic), but more studies are needed
Author of this blog Bert Kerkhof writes about health care and youth care

Waardeer dit blog
Dit artikel las je gratis. De moeite waard? Laat je waardering zien en draag €1 bij of een veelvoud daarvan. Via Paypal of creditcard.
€ 1,00


Plaats een reactie